
Coaching the female athlete
- milesandmacros
- Mar 12, 2021
- 4 min read


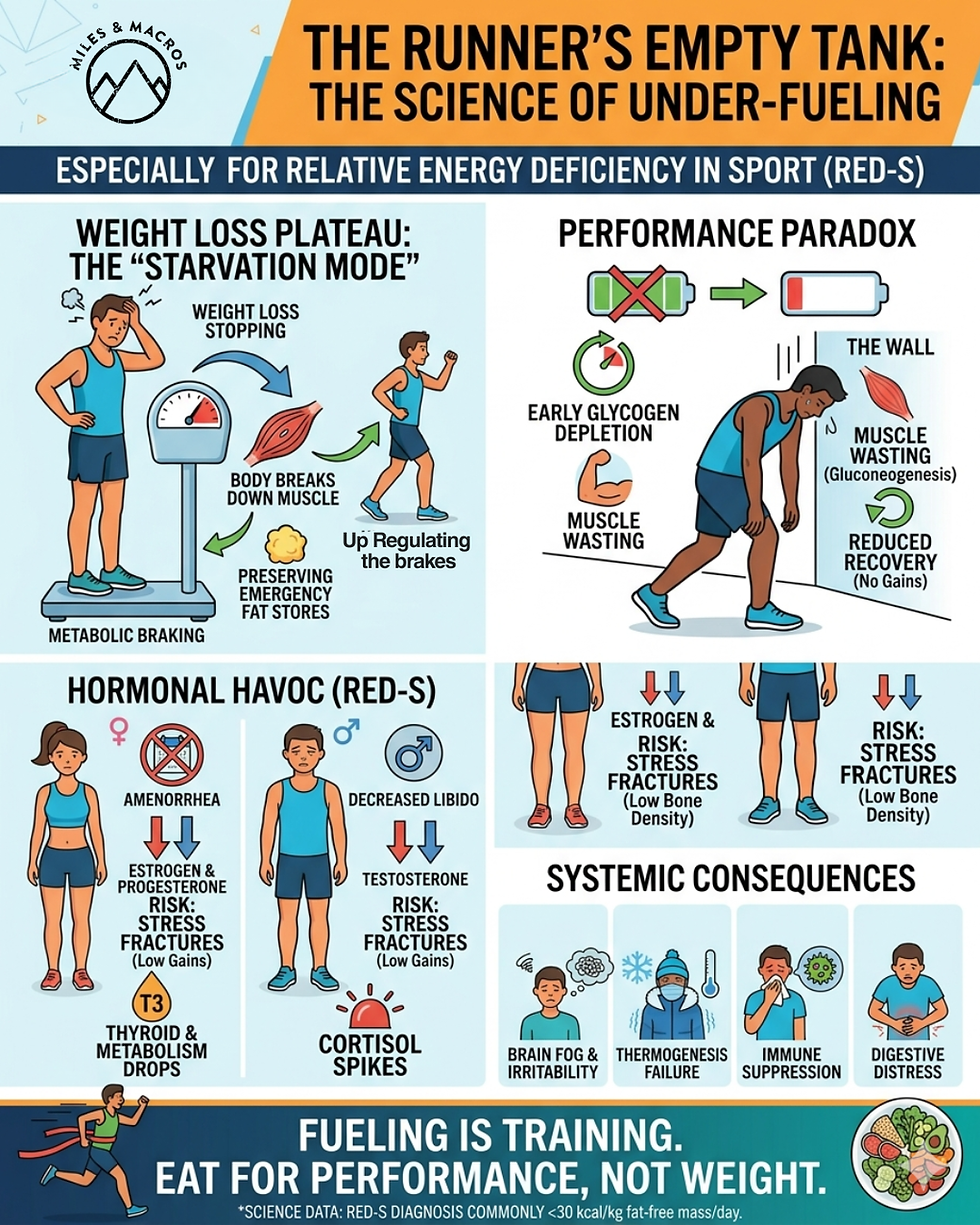
The immediate differences that distinguishes female athletes from male athletes is usually focused on the body size and organ differences. However, the lifespan of the menstrual cycle provides many further distinguishing factors for the female athlete. The female's hormonal fluctuation influences both performance (i.e. muscle strength, time to fatigue, etc.) and physiological responses to exercise (i.e. blood lactate production, carbohydrate metabolism, and heart rate). Factors that need to be considered for exercise regimes should focus on the low/high pre/postmenopausal women in order to avoid the ‘Female Athlete Triad’ of disordered eating, osteoporosis, and amenorrhea. The Female Athlete Triad: *Amenorrhea (period loss) *Osteoporosis (low bone mineral density) *Disordered Eating (low energy availability) with or without an eating. ~~ONLY ONE symptom of the triad is needed for the diagnosis.~~ Early detection of these symptoms is important, as each component of the triad can have irreversible consequences and may increase in severity.
Coaches play an imperative role in the prevention of the female athlete triad and possess the ability to positively impact female athletes by educating and supporting them to adopt healthy patterns of behavior. Coaching athletes is a very individualized process - no one athlete is like the other. Often this is why athletes gravitate towards private, personalized coaching in the first place. Group training (only*) does not provide an individual with the specific tools to fine tune THEIR skills nor the singular focus on the athlete's training, nutrition, or recovery. Another component of private coaching, that is often overlooked, is the extra needs of the female athlete. The females' need for training is much more complex than a males' need for training when it comes to biological/reproductive differences. The gender specific physiological, anatomical, psychological, performance fluctuations associated with menstrual cycle, menopause, and social aspects of the female athlete play a major factor in how training plans and nutrition should be set up. For simplicity, I have broken the female athlete's career into two "stages" and the complexities that enter into each stage. Prepubescent/Young Adolescents: According to www.globalsportsdevelopment.org, "A survey of eighty high school athletes found that 78% of the respondents had one or more of these conditions". Young female athletes in high school track & field/cross country are in the middle of their early developmental stages. The greatest increase in bone mass happens during puberty; ages 11 and 14 years of age (ncbi.com). Often disordered eating and amenorrhea go together. Consistent hard training sessions, social pressures, and competitiveness to win are all major stressors. The stressors on weight/size is high and often females mistakenly see leanness as a way to enhance sport performance. Some females that participate in competitive sports may never even get their first period because they've been training so hard and others that may get their periods, but lose them once they increase their training and change their eating habits. Estrogen is lower in girls with female athlete triad. Low estrogen levels accompanied with poor nutrition/calcium, can lead to osteoporosis, another aspect of the triad. Osteoporosis is loss of bone density and improper bone formation. With poor bone density the athlete will get more stress fractures. Calcium deficiency now can also have effects on just how strong a woman's bones are later in their lives. When building up mileage, coaches should try to organize the training weeks around the menstrual cycle, such that increases in the volume of training correlate with the latter part of the follicular phase. The follicular phase is when the estrogen level is high. The athlete should avoid doing threshold workouts around menstruation. If the athlete doesn’t feel well or is bloated (from the drop in progesterone going from the luteal phase to the follicular phase) she should not push herself. Middle Aged: Females entering/in menopause have lower energy levels and bone density. The focus on staying injury free and recovery is extremely important. The severity and duration of symptoms of menopause widely impact performance and are hugely variable. The physiological impact of menopause alone may affect a woman's running and injury risk. Coaches must be mindful of this when treating peri-menopausal women. Most women begin menopause between the ages of 45 and 55 years - the average being 51 years of age. The effect of estrogen's effects on tendons and ligaments is still very misunderstood; however, research implies that estrogen has protective benefits for connective tissue tensile strength, healing, and ability to load-bear. 95% of collagen in tendons is attributed to Type 1 collagen. As we can see with normal skin ageing and other muscular-skeletal conditions, age reduces collagen and connective tissue’s ability to repair. Studies suggest a connection between declining estrogen and pelvic prolapse (a process associated with pelvic ligaments and collagen content of surrounding tissue) (Le Blanc et al, 2017). Potential collagen changes with menopause highlight the need to not only consider changes to the commonly problematic gluteal, posterior tibial, and Achilles tendons, but also the need to address abdominal and pelvic floor changes. Another reason to continue pelvic floor exercises! Estrogen plays an important role in the growth and maturation of bone as well as in the regulation of bone turnover in adult bone. Women can lose up to 20% of their bone density in the first 5-7 years post menopause, as estrogen levels drop (NHS website: Menopause and your bone health). Muscle strength losses peri and post menopause are well documented. Recent CSP promotional material quotes up to 8% muscle strength loss per decade from the age of 30 if no steps are taken to counteract this. A recent Finnish study (Bondarev et al, 2018) of over 900 women showed menopausal status is significantly associated with reduced muscle strength, power and vertical jump height.

Above is a chart from "The Female Athlete Triad: An Emerging Role for Physical Therapy" by Paula E. Papanek, MPT, PhD, ATC, FACSM1. https://www.jospt.org/doi/pdf/10.2519/jospt.2003.33.10.594
Note: Long-distance female runners feel the social pressures that they need to fit in by having muscular quads, a six pack, and be feminine for society. This addresses the idea of hegemonic femininity, which speaks to the idea that a woman must conform to a certain role (which includes being emotional, passive, dependent, maternal, compassionate, and gentle) in order to be perceived as a traditional woman by society. The pressures to "look the part" can introduce athletes towards malnutrition. With all of these pressures and intertwined with the aspect of athletic competition the risk of Female Triad syndrome increases.


Comments